
What Does SBAR Stand For?
SBAR stands for Situation, Background, Assessment, Recommendation. It’s a standardized communication framework used by nurses and healthcare professionals to share critical patient information clearly and efficiently.
- Situation – What’s happening right now
- Background – Clinical context and history
- Assessment – Your professional evaluation
- Recommendation – What you think should be done
SBAR is the gold standard for clinical communication in nursing, used in hospitals, clinics, and healthcare facilities worldwide. This guide explains what SBAR means, why it’s important, and how to use it effectively in your nursing practice.
Quick Facts About SBAR
- Full Form: Situation, Background, Assessment, Recommendation
- Origin: Developed by U.S. Navy, adapted for healthcare by Kaiser Permanente
- Primary Use: Nurse-to-physician communication, shift handoffs, emergencies
- Benefits: Reduces communication errors by 30%, improves handoff efficiency
- Adoption: Used in 80%+ of U.S. hospitals, required by Joint Commission
The Four Components of SBAR
S – Situation
What’s happening right now?
The Situation describes the current patient condition or the reason for your communication. Be concise and specific.
What to include:
- Patient name and location
- Chief complaint or current problem
- Vital signs if abnormal
- Changes in patient status
- Your level of concern
Example: “This is Sarah calling from 4 West about Mr. Johnson in room 412. He’s experiencing increased shortness of breath and his oxygen saturation has dropped to 88% on room air.”
B – Background
What’s the clinical context?
The Background provides relevant medical history and context that helps the listener understand the current situation.
What to include:
- Admitting diagnosis
- Relevant medical history
- Current medications
- Recent procedures or treatments
- Pertinent lab results
- Allergies
Example: “Mr. Johnson was admitted two days ago with pneumonia. He has a history of COPD and is on 2L oxygen at baseline. He received his last dose of antibiotics at 0800. His most recent chest X-ray showed bilateral infiltrates.”
A – Assessment
What do you think is going on?
The Assessment is your professional evaluation of the situation. This is where you use your clinical judgment and nursing expertise.
What to include:
- Your clinical impression
- Severity of the situation
- Your professional concern level
- What you think might be causing the problem
- Comparison to baseline status
Example: “I’m concerned his pneumonia may be worsening despite antibiotic therapy. His respiratory status has declined over the past two hours, and he’s now requiring more oxygen support. He appears more lethargic than earlier today.”
R – Recommendation
What do you think should be done?
The Recommendation states what you think needs to happen next. Be specific and assertive about what you’re requesting.
What to include:
- Specific actions you’re requesting
- Urgency level (routine, soon, immediately)
- Tests or treatments you think are needed
- Timeline for intervention
- Follow-up plan
Example: “I’d like you to evaluate him now. Should we get a stat chest X-ray and arterial blood gas? I think he may need increased oxygen support or possibly transfer to ICU. Can you come assess him within the next 30 minutes?”
SBAR Examples in Nursing Practice
Example 1: Calling a Physician About Patient Deterioration
S: “Dr. Smith, this is Maria from ICU calling about Mrs. Rodriguez in bed 3. Her blood pressure has dropped to 82/50 and she’s become increasingly lethargic over the past hour.”
B: “She’s post-op day 2 from a bowel resection. She’s been on IV fluids at 125 mL/hour. Her last hemoglobin was 8.2 this morning. She has a history of GI bleeding. Her urine output has decreased to 15 mL this past hour.”
A: “I’m concerned she may be bleeding internally. Her abdomen is more distended than earlier, and her drain output has increased to 200 mL this shift and looks darker than before. She’s showing signs of hypovolemia.”
R: “I think we need to check a stat hemoglobin and type and cross for 2 units of blood. Should we also get a CT scan of her abdomen? I’d like you to come evaluate her immediately. Should I notify the OR that we may need to take her back?”
Example 2: Nurse-to-Nurse Shift Handoff
S: “Mr. Thompson in room 215 is a 68-year-old admitted for chest pain, currently stable on telemetry with no events this shift.”
B: “He came in yesterday with atypical chest pain. Troponins were negative times three. EKG showed no acute changes. He has a cardiac catheterization scheduled for tomorrow morning at 0700. He’s NPO after midnight. IV access is a 20-gauge in his right forearm, patent and flushing well.”
A: “He’s been pain-free for the past 12 hours. All vital signs are stable and within normal limits. He’s anxious about the procedure tomorrow but otherwise doing well. No changes in cardiac rhythm on telemetry.”
R: “Continue telemetry monitoring overnight. Remind him about NPO status at 2300. His wife wants to speak with the cardiologist before the procedure – she’ll be here at 0630. He’s due for his morning medications but hold them until after the cath per cardiology.”
Example 3: Rapid Response Situation
S: “Rapid response called for Mr. Lee in room 320. He’s unresponsive with a heart rate of 38 and blood pressure 70/40.”
B: “72-year-old male, admitted yesterday for syncope. History of complete heart block, pacemaker placed 5 years ago. Takes metoprolol 50mg twice daily, last dose at 0800. He was alert and oriented 10 minutes ago.”
A: “I think his pacemaker has failed. He was fine during my last check, now he’s unresponsive with severe bradycardia. His rhythm on the monitor shows no pacing spikes.”
R: “We need atropine 0.5mg IV now and pacemaker interrogation stat. Call cardiology for emergent consult. Anesthesia should be notified for possible temporary pacing. I’ve already started a second IV and we’re preparing transcutaneous pacing pads.”
Example 4: Medication Concern
S: “Dr. Jones, this is Kevin calling about Mrs. Patterson in 518. I’m calling about her new digoxin order – her heart rate is 52 and the order is for 0.25mg.”
B: “She’s a 79-year-old admitted with atrial fibrillation. She’s been on diltiazem 30mg four times daily. Her potassium this morning was 3.2. She has no prior history of digoxin use.”
A: “I’m concerned about giving digoxin with her heart rate already in the 50s and her low potassium level. The combination of diltiazem and digoxin might cause excessive bradycardia.”
R: “Should we hold the digoxin until you can reassess? Do you want to recheck her potassium and correct it first? Should we consider holding or reducing her diltiazem dose?”
When to Use SBAR in Nursing
SBAR should be used in these common nursing situations:
Calling Physicians
- Reporting changes in patient condition
- Requesting new orders or interventions
- Discussing abnormal lab or test results
- Urgent or emergency situations
- Medication clarifications
Shift Handoffs
- Nurse-to-nurse bedside report
- Transfer between units or floors
- Patient handoff to OR or procedures
- Discharge communication to home health
- Admission reports from ED or PACU
Team Communication
- Interdisciplinary rounds
- Code Blue situations
- Rapid response team activations
- Care conferences with families
- Quality improvement discussions
Documentation
- Progress notes in EHR
- Incident or safety event reports
- Transfer summaries
- Communication logs
- Peer consultation notes
Best Practices for Using SBAR
Be Prepared
Have the patient’s chart, vital signs, and relevant lab results in front of you before making the call. Write down your SBAR points if needed. Know what you’re going to say before you pick up the phone.
Be Concise
Stick to relevant information only. Your entire SBAR communication should take 1-2 minutes maximum in most situations. Don’t include unnecessary details that don’t relate to the current issue.
Be Specific
Use exact numbers, times, and measurements. Say “blood pressure 82/50” not “low blood pressure.” Say “oxygen saturation 88%” not “low O2 sat.” Precision matters.
Be Confident
SBAR gives you a structure to speak assertively with physicians and other providers. Your assessment and recommendation are valuable – share them clearly without apologizing.
Use Clinical Judgment
The Assessment section is where your nursing expertise shines. Don’t be afraid to share your professional opinion about what you think is happening with the patient.
Follow Up
After giving your Recommendation, confirm what will happen next. Document the conversation including who you spoke with, when, and what was decided. Close the loop.
Practice Regularly
Use SBAR even for routine communications. The more you practice, the more natural it becomes. New nurses should practice SBAR with colleagues before making high-stakes calls.
Adapt as Needed
While SBAR provides structure, adapt it to the urgency of the situation. In a code, lead with the critical information. For routine updates, you can be more thorough.
Common SBAR Mistakes to Avoid
Being Too Vague
Wrong: “The patient isn’t doing well.”
Right: “Mr. Smith’s oxygen saturation dropped to 88% on 2L nasal cannula and his respiratory rate increased to 28.”
Why it matters: Vague descriptions don’t give the physician enough information to make decisions.
Including Irrelevant Information
Wrong: Sharing the patient’s entire admission history when calling about an acute issue.
Right: Share only background information directly relevant to the current situation.
Why it matters: Too much information wastes time and buries the critical details.
Skipping the Assessment
Wrong: Only reporting objective facts without your clinical evaluation.
Right: “I’m concerned this may be sepsis based on the fever of 102.8, heart rate of 118, and altered mental status.”
Why it matters: Your clinical judgment adds value – physicians want to know what you think.
Not Making a Recommendation
Wrong: Ending with “What do you want me to do?”
Right: “I think we should start IV fluids, get blood cultures, and administer antibiotics now.”
Why it matters: You’re the one with the patient – suggest what you think needs to happen.
Being Unprepared
Wrong: Calling without having the chart or vital signs available.
Right: Gather all relevant information before initiating the call.
Why it matters: Being unprepared wastes everyone’s time and delays patient care.
Using Apologetic Language
Wrong: “I’m sorry to bother you, but…”
Right: “I’m calling about Mrs. Johnson. Her condition has changed and I need you to evaluate her.”
Why it matters: You’re advocating for your patient – be confident, not apologetic.
SBAR Template for Nurses
Quick Reference Guide – Print and Keep in Your Pocket
Use this template to prepare before calling physicians or during handoffs:
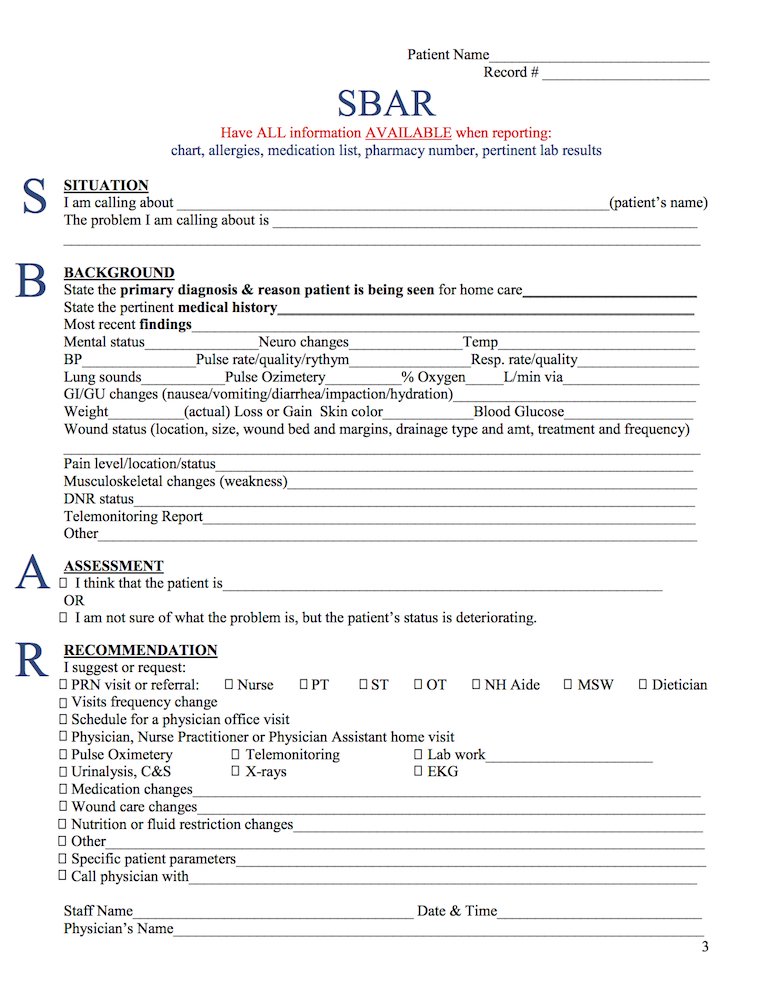
S – SITUATION
- I’m calling about ________________ in ________________
- The problem is ________________
- Vital signs: BP _____ HR _____ RR _____ Temp _____ O2 sat _____
- My concern level is: ☐ Routine ☐ Urgent ☐ Emergency
B – BACKGROUND
- Admitting diagnosis: ________________
- Relevant history: ________________
- Current medications: ________________
- Recent labs/tests: ________________
- Allergies: ________________
A – ASSESSMENT
- I think the problem is ________________
- I’m concerned about ________________
- The patient is: ☐ Stable ☐ Unstable ☐ Deteriorating
- This is different from baseline because ________________
R – RECOMMENDATION
- I recommend ________________
- I need you to ________________
- Timeframe: ☐ When available ☐ Within 1 hour ☐ Immediately
- I have already done ________________
Want a printable PDF version? Download our free SBAR Pocket Card to keep in your badge holder.
SBAR vs Other Communication Frameworks
| Framework | Components | Best Used For | Key Difference |
| SBAR | Situation, Background, Assessment, Recommendation | Physician calls, handoffs, urgent situations, general nursing communication | Most widely adopted, includes nurse’s recommendation |
| ISBAR | Identify, Situation, Background, Assessment, Recommendation | When patient identity verification is critical | Adds explicit patient identification step at beginning |
| IPASS | Illness severity, Patient summary, Action list, Situational awareness, Synthesis | Pediatric handoffs, complex patients | More detailed, pediatric-focused, includes action items |
| SOAP | Subjective, Objective, Assessment, Plan | Written documentation in medical records | Documentation format, not designed for verbal communication |
| AIDET | Acknowledge, Introduce, Duration, Explanation, Thank | Patient-facing communication, customer service | Focuses on patient experience, not clinical handoffs |
Why SBAR Is Effective
Reduces Cognitive Load
The structured format reduces the mental effort required to organize information during stressful situations. Both parties know what to expect and in what order.
Creates Shared Mental Model
SBAR ensures both the nurse and physician have the same understanding of the patient’s situation, reducing misinterpretation and miscommunication.
Empowers Nurses
By requiring an Assessment and Recommendation, SBAR validates nursing expertise and encourages nurses to think critically and advocate for patients.
Saves Time
Studies show SBAR communications are 40% faster than unstructured conversations while conveying more complete information.
Improves Patient Outcomes
Research demonstrates that hospitals using SBAR see 30% fewer communication-related adverse events and improved patient safety metrics.
Meets Regulatory Standards
The Joint Commission requires standardized handoff communication. SBAR satisfies this requirement and is recognized as a best practice.
SBAR Tips for New Nurses
If you’re new to using SBAR, these strategies will help you build confidence:
Write It Down First
Before calling a physician, write out your SBAR. This gives you a script to follow and ensures you don’t forget critical information.
Practice with Colleagues
Role-play SBAR scenarios with experienced nurses during downtime. Practice builds confidence and helps you refine your communication style.
Start with Non-Urgent Calls
Use SBAR for routine communications first (lab results, discharge orders). Once comfortable, apply it to urgent situations.
Keep a Pocket Card
Print the SBAR template and keep it in your badge holder or pocket. Having a visual reminder helps until it becomes second nature.
Don’t Apologize
Never start with “I’m sorry to bother you.” You’re calling about patient care – that’s your job and it’s important.
Ask for Feedback
After SBAR calls, ask your preceptor or charge nurse for feedback. Continuous improvement makes you a better communicator.
SBAR Across Different Healthcare Settings
ICU/Critical Care
In critical care, SBAR is used for rapid response situations, ventilator changes, hemodynamic instability, and family conferences. Speed and precision are essential.
Focus: Immediate threats to life, trending vital signs, vasopressor adjustments
Medical-Surgical Units
Med-surg nurses use SBAR for routine physician calls, transfers, and changes in patient status. It’s the most common application of SBAR.
Focus: Pain management, lab results, discharge planning, new symptoms
Emergency Department
ED staff use SBAR for trauma activations, critical patients, and transfers to inpatient units. Communication must be rapid but complete.
Focus: Mechanism of injury, time-sensitive interventions, disposition planning
Operating Room
Perioperative teams use SBAR for surgical timeouts, handoffs to PACU, and intraoperative complications.
Focus: Surgical site verification, anesthesia concerns, blood loss, specimens
Long-Term Care
LTC facilities use SBAR when calling physicians about resident changes, often by phone without in-person physician presence.
Focus: Baseline comparison, falls, skin breakdown, behavioral changes
Home Health
Home health nurses use SBAR to communicate with physicians remotely about patient status and care plan changes.
Focus: Wound status, medication compliance, caregiver concerns, environmental safety
Summary
SBAR (Situation, Background, Assessment, Recommendation) is the gold standard communication framework in nursing and healthcare. It provides a structured, efficient method for sharing critical patient information during physician calls, shift handoffs, rapid responses, and interdisciplinary communication.
By using SBAR consistently, nurses improve patient safety, reduce communication errors, save time, and demonstrate professional expertise. The framework empowers nurses to speak confidently with physicians and other providers while ensuring complete, organized information transfer.
Whether you’re a new graduate or an experienced nurse, mastering SBAR is essential for effective clinical communication. Practice regularly, use the template when needed, and remember that your Assessment and Recommendation are valuable contributions to patient care.
Ready to improve your SBAR skills? Download our free SBAR pocket card template and start practicing today.
Common Questions About SBAR
What does SBAR stand for?
SBAR stands for Situation, Background, Assessment, Recommendation. This acronym represents a four-step communication framework that helps healthcare professionals share patient information in a clear, organized manner. SBAR was originally developed by the U.S. Navy for submarine crews and adapted for healthcare by Kaiser Permanente to reduce communication errors and improve patient safety.
What is SBAR in nursing?
In nursing, SBAR is a structured communication tool used when reporting patient status to physicians, during shift handoffs, in emergency situations, and when transferring patients between units. It ensures that critical information is communicated consistently and completely, reducing the risk of miscommunication that could compromise patient safety. Nurses use SBAR daily for physician calls, rapid response situations, and interdisciplinary team communication.
What does SBAR mean in healthcare?
In healthcare settings, SBAR means using a standardized format to communicate patient information: Situation (current patient status), Background (relevant medical history), Assessment (clinical evaluation), and Recommendation (suggested actions). This framework is used across all healthcare disciplines including nursing, medicine, pharmacy, respiratory therapy, and allied health professions to ensure consistent, complete communication.
Why is SBAR important in nursing?
SBAR is important in nursing because it:
- Reduces communication errors – Standardized format prevents missed information
- Improves patient safety – Critical details are communicated consistently
- Saves time – Organized structure makes handoffs faster and clearer
- Empowers nurses – Provides confidence when speaking with physicians
- Meets Joint Commission standards – Satisfies regulatory requirements for handoff communication
- Reduces sentinel events – Studies show 30% reduction in communication-related errors
What is SBAR communication?
SBAR communication is a structured conversation format that follows four steps: describing the current Situation, providing relevant Background, sharing your clinical Assessment, and making a Recommendation for action. This method ensures that both parties have the same information and understand what needs to happen next. It typically takes 1-2 minutes and creates a shared mental model between healthcare providers.
What does SBAR stand for?
SBAR stands for Situation, Background, Assessment, Recommendation. This acronym represents a four-step communication framework that helps healthcare professionals share patient information in a clear, organized manner. SBAR was originally developed by the U.S. Navy and adapted for healthcare to reduce communication errors and improve patient safety.
What is SBAR in nursing?
In nursing, SBAR is a structured communication tool used when reporting patient status to physicians, during shift handoffs, in emergency situations, and when transferring patients between units. It ensures that critical information is communicated consistently and completely, reducing the risk of miscommunication that could compromise patient safety.
What does SBAR mean in healthcare?
In healthcare settings, SBAR means using a standardized format to communicate patient information: Situation (current patient status), Background (relevant medical history), Assessment (clinical evaluation), and Recommendation (suggested actions). This framework is used across all healthcare disciplines including nursing, medicine, pharmacy, and allied health professions.
Why is SBAR important in nursing?
SBAR is important in nursing because it reduces communication errors, improves patient safety, saves time, empowers nurses, and meets Joint Commission standards for handoff communication. The standardized format prevents missed information and ensures critical details are communicated consistently.
What is SBAR communication?
SBAR communication is a structured conversation format that follows four steps: describing the current Situation, providing relevant Background, sharing your clinical Assessment, and making a Recommendation for action. This method ensures that both parties have the same information and understand what needs to happen next






{kind=link}